Health Insurance Claim Form 1500 Printable
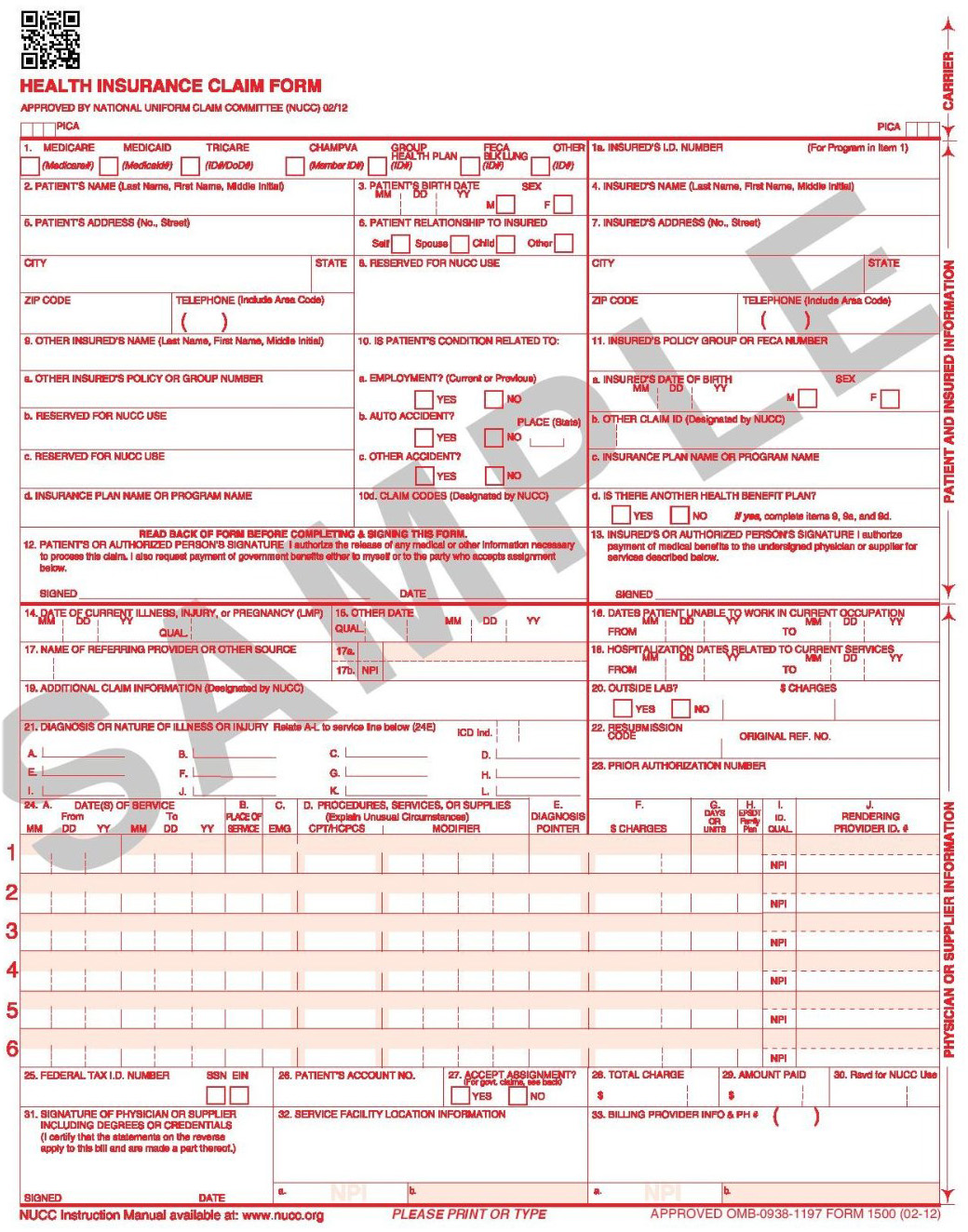
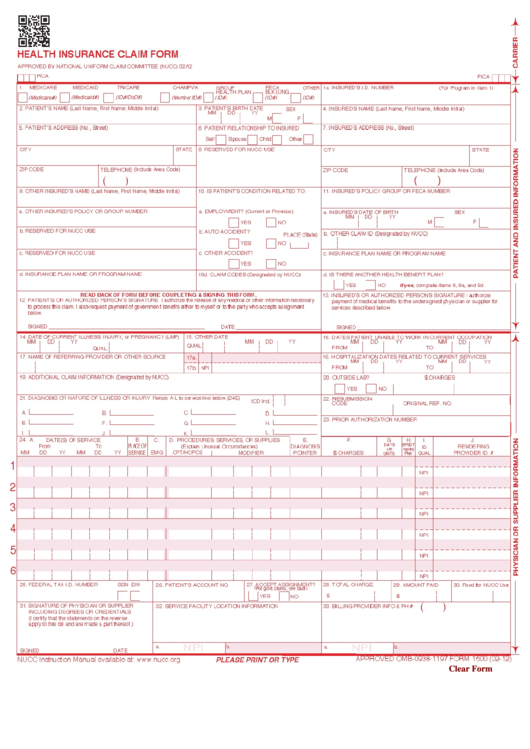
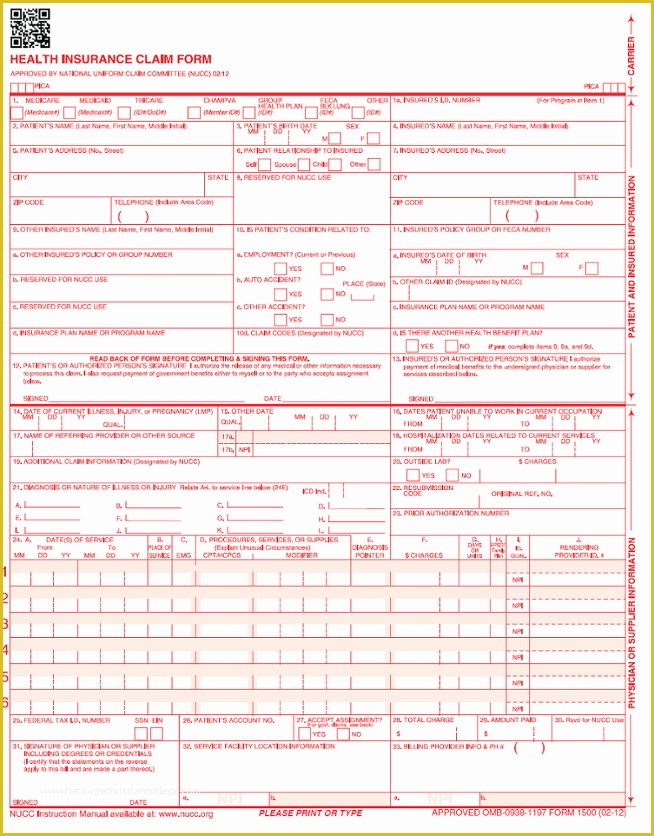
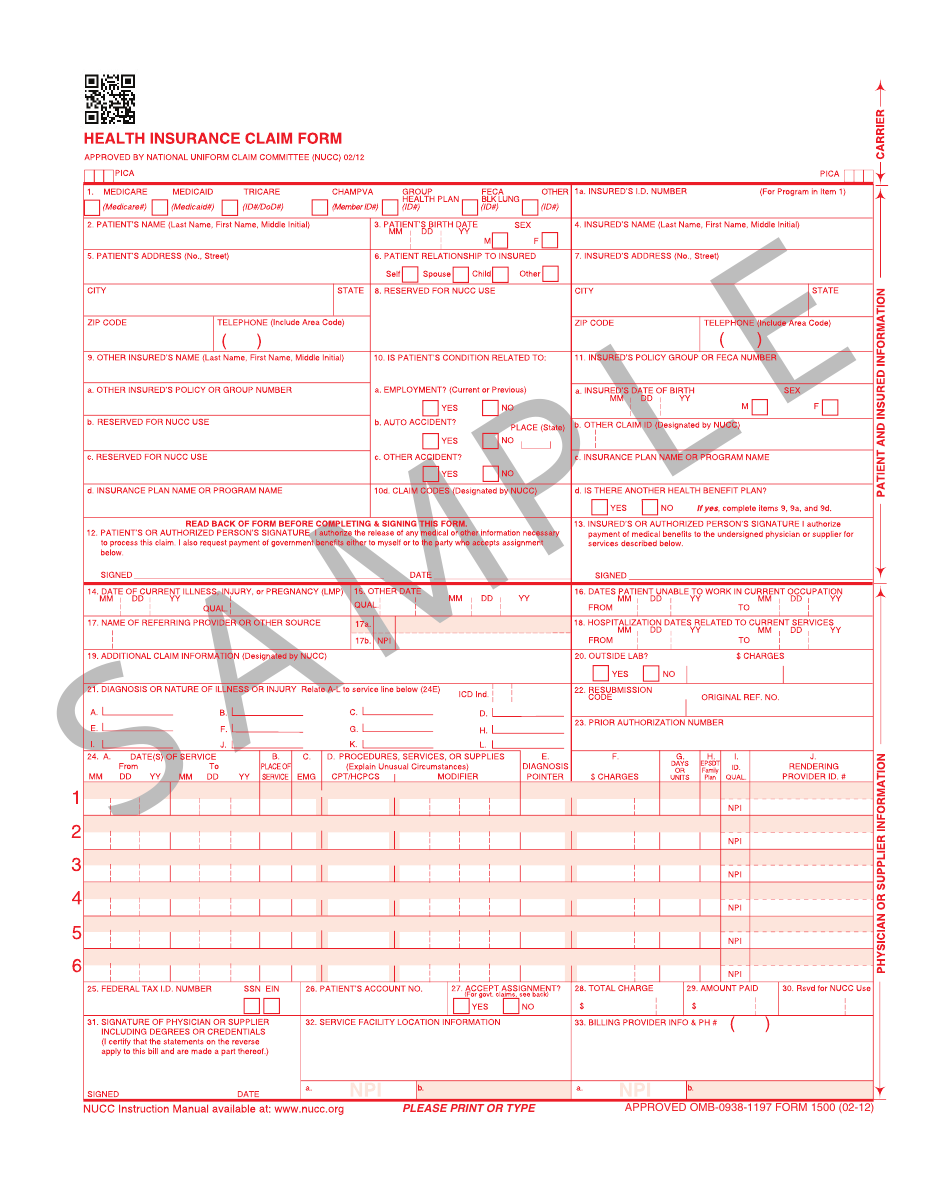
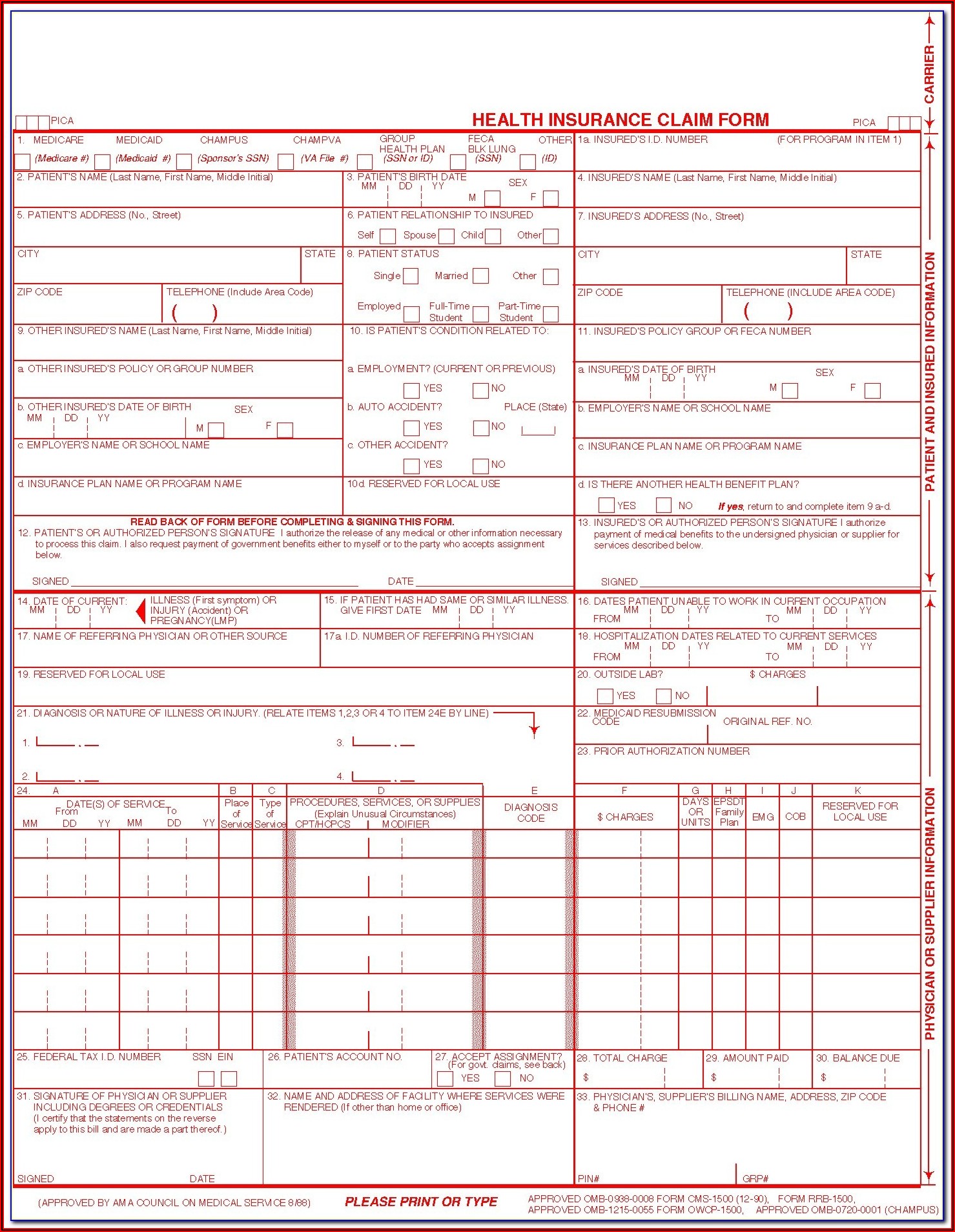
Health Insurance Claim Form 1500 Printable - Web reset form print form 1500 health insurance claim form approved by national uniform claim committee 08/05. Health insurance claim form keywords: Web there are two primary ways of submitting a health insurance claim: Web please print or type. We only accept claim forms printed in flint ocr red, j6983, (or exact match) ink. Number (for program in item 1) 4. Insured's address (no., street) city state. It provides information about the client, their corresponding insurance policy, and their diagnosis and treatment. Patient ’s or authorized person s signature i authorize the release of any medical or other information necessary. The template ensures that all. Insured's name (last name, first name, middle initial) 7. You can also use your computer to complete this form and then print it out to mail it. Begin by obtaining itemized receipts. Review everything to make sure it is correct prior to filing. Web health insurance claim form 1. (medicare#) (medicaid#) (id#/dod#) (member id#) (id#) (id#) Number (for program in item 1) 4. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. Web please print or type. Web health. Download or email cms 1500 & more fillable forms, register and subscribe now! Health insurance claim form keywords: Insured's name (last name, first name, middle initial) 7. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. Department of health & human services. When you receive your explanation of medicare benefits papers, attach copies to your hcfa 1500 claim forms. Insured's name (last name, first name, middle initial) 7. Health, insurance, claim, form created date: Web there are two primary ways of submitting a health insurance claim: Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac),. Web there are two primary ways of submitting a health insurance claim: Insured's name (last name, first name, middle initial) 7. It can be purchased in any version required by calling the u.s. Sign up to get the latest information about your choice of cms topics. Web cms 1500 is a claim form for health insurance. Web health insurance claim form 1. Web there are two primary ways of submitting a health insurance claim: Make copies of everything that you plan to submit to the health insurance company. Web please print or type. (medicare#) (medicaid#) (id#/dod#) (member id#) (id#) (id#) The system needs the colors for automated form reading. To ensure faster processing of your claim, be sure to do the following: Medicare medicaid champus champva other read back of form before completing & signing this form. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office. Web health insurance claim form 1. Patient ’s or authorized person s signature i authorize the release of any medical or other information necessary. Please mail them to the name and address listed here. Web please print or type. Medicare medicaid champus champva other read back of form before completing & signing this form. Department of health & human services. You can also use your computer to complete this form and then print it out to mail it. Web please print or type. Web health insurance claim form 1. The system needs the colors for automated form reading. Obtain the proper claim form for your specific health insurance company. Web health insurance claim form 1. Health, insurance, claim, form created date: Download or email cms 1500 & more fillable forms, register and subscribe now! (medicare#) (medicaid#) (id#/dod#) (member id#) (id#) (id#) Insured's address (no., street) city state. Medicare medicaid tricare champva other read back of form before completing & signing this form. Sign up to get the latest information about your choice of cms topics. The system needs the colors for automated form reading. Make copies of everything that you plan to submit to the health insurance company. Web cms 1500 is a claim form for health insurance. Obtain the proper claim form for your specific health insurance company. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. It was originally used to claim billing by either suppliers or a physician. Health, insurance, claim, form created date: Number (for program in item 1) 4. Insured's name (last name, first name, middle initial) 7. Health insurance claim form subject: It provides information about the client, their corresponding insurance policy, and their diagnosis and treatment. Web health insurance claim form 1. Web please print or type. Patient ’s or authorized person s signature i authorize the release of any medical or other information necessary. Department of health & human services. Review everything to make sure it is correct prior to filing. Health insurance claim form keywords: Insured's address (no., street) city state. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers,. It can be purchased in any version required by calling the u.s. Health, insurance, claim, form created date: Web cms 1500 dynamic list information. Department of health & human services. It provides information about the client, their corresponding insurance policy, and their diagnosis and treatment. It was originally used to claim billing by either suppliers or a physician. You can also use your computer to complete this form and then print it out to mail it. Web health insurance claim form 1. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. Begin by obtaining itemized receipts. If you write on the form, use black or blue ink and print clearly and legibly. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. The system needs the colors for automated form reading. Number (for program in item 1) 4.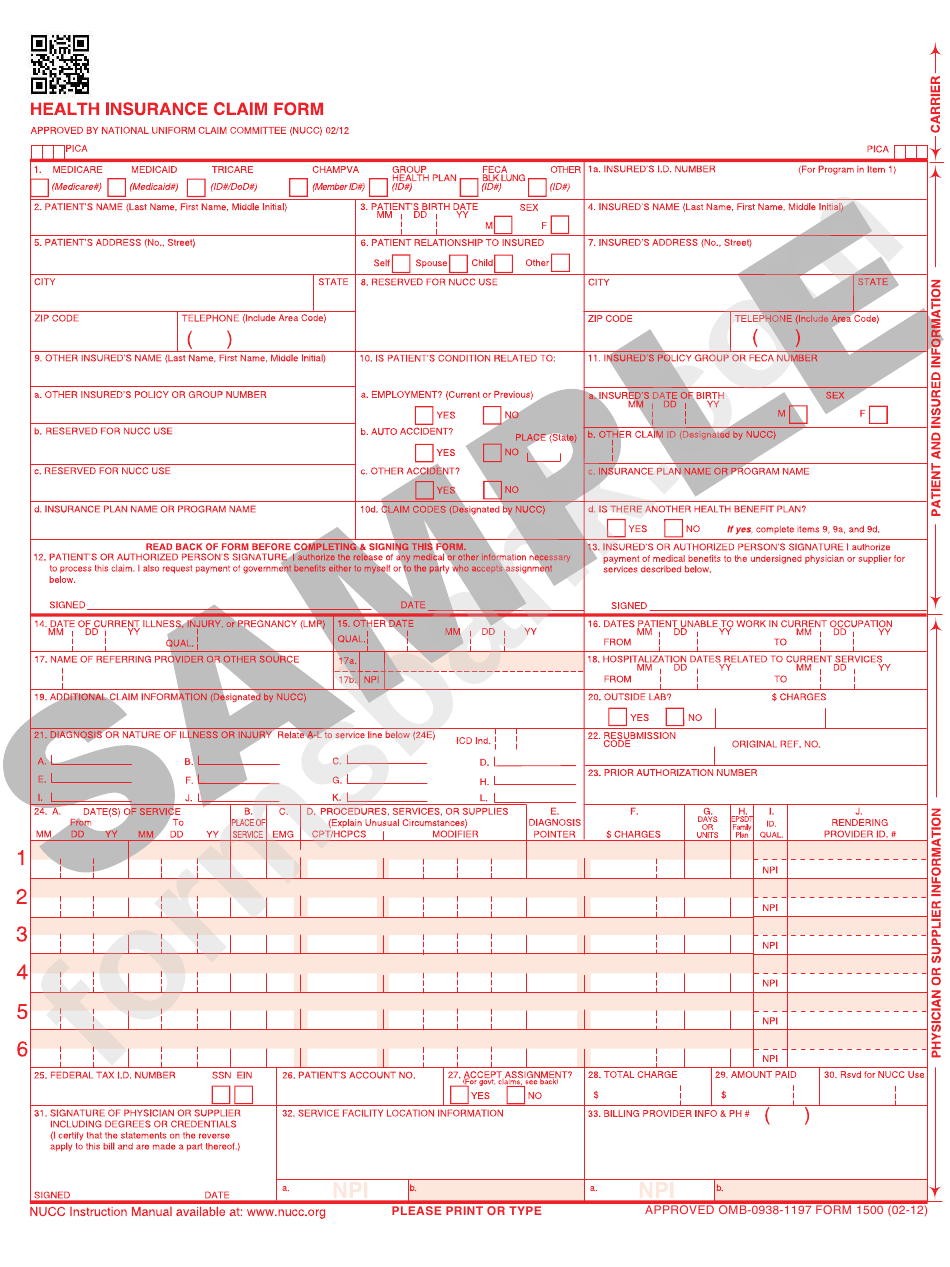
Health Insurance Claim Form Printable Pdf Download Gambaran
Insurance Claim Form Printable Pdf Download Gambaran
Free Printable 1500 Medical Claim Form Printable Forms Free Online
Fillable Form 1500 Health Insurance Claim Form printable pdf download
Free Fillable Cms 1500 Claim Forms Printable Forms Free Online
Free Health Insurance Claim Form 1500 Template Printable Templates

2005 Form CMS 1500 Fill Online, Printable, Fillable, Blank PDFfiller
Fillable 1500 Claim Form Free Form Resume Examples l6YNvp3Y3z

Ghi Claim Form 1500 1stglobaldesign

HCFA Forms, CMS 1500 Medical Forms, Health Insurance Claim Forms
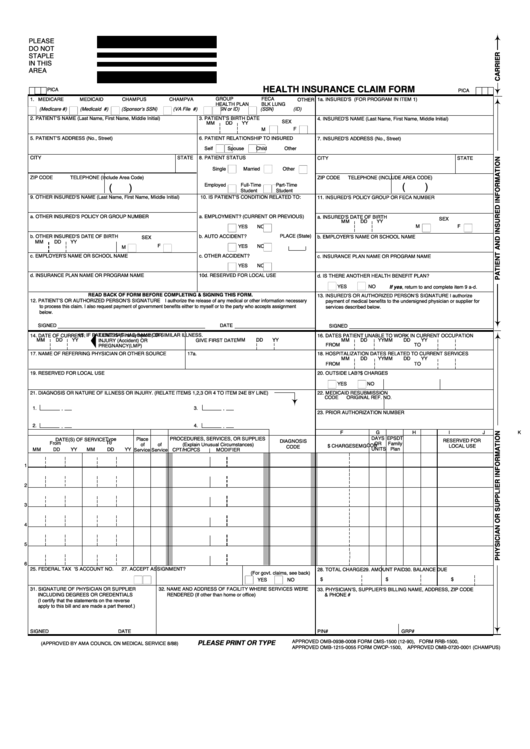
Medicare Medicaid Tricare Champva Other Read Back Of Form Before Completing & Signing This Form.
Web There Are Two Primary Ways Of Submitting A Health Insurance Claim:
Web The 1500 Health Insurance Claim Form (1500 Claim Form) Answers The Needs Of Many Health Care Payers.
Web Reset Form Print Form 1500 Health Insurance Claim Form Approved By National Uniform Claim Committee 08/05.
Related Post: